Intervertebral Disc Disease (IVDD) is one of the most common spinal disorders in dogs, characterized by the degeneration and subsequent herniation or extrusion of the intervertebral disc material, leading to spinal cord compression and neurological dysfunction
The disease is classified into Hansen Type I and Hansen Type II disc disease, based on the nature and progression of disc degeneration
In Hansen Type I IVDD, as observed in this case, the nucleus pulposus undergoes chondroid degeneration and becomes calcified. Sudden extrusion of this degenerated material through the annulus fibrosus results in acute spinal cord compression, inflammation, and occasionally hemorrhage
Zeus presented to our clinic with an acute onset of severe neck pain and marked ventroflexion of the head. The patient was non-ambulatory and unable to bear weight on all four limbs, indicating complete tetraparesis.
Neurological examination revealed UMN deficits with loss of proprioception in his 4 limbs (non-ambulatory) urine retention and constipation, with normal LMN reflexes So, lesion is localized from C1-C5
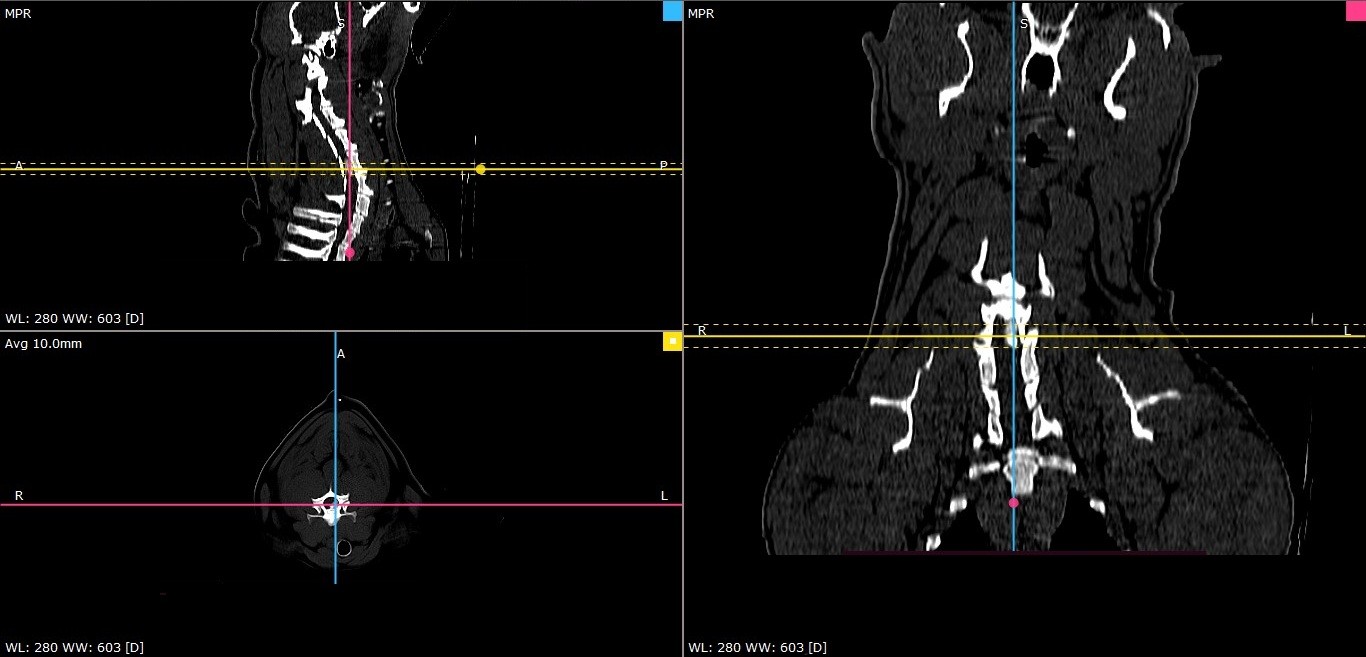
Zeus was submitted for Cervical CT scan CT revealed disc extrusion (Hansen type 1) between C5-C6 with 66% spinal compression with intra-dural hemorrhage.
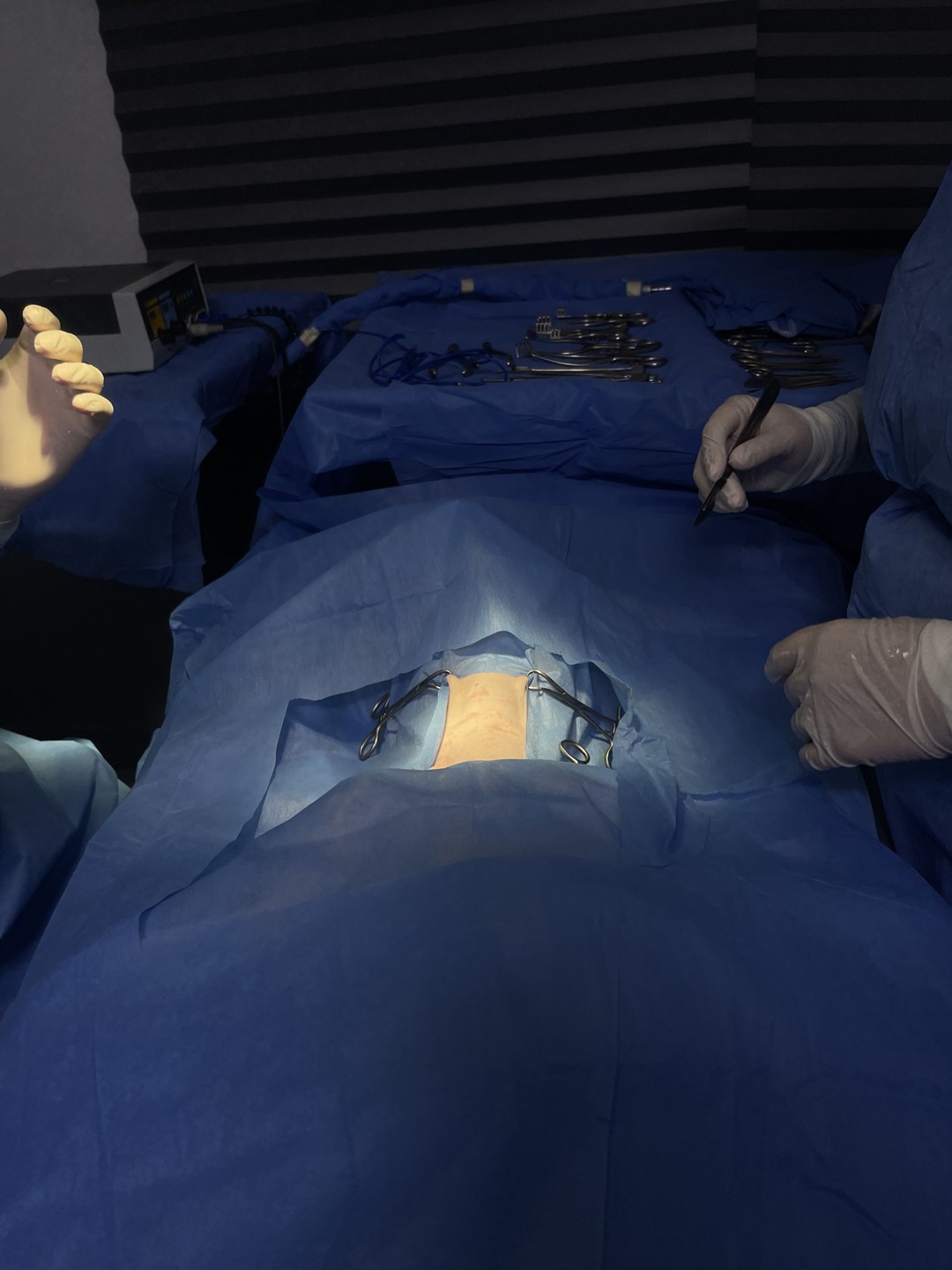
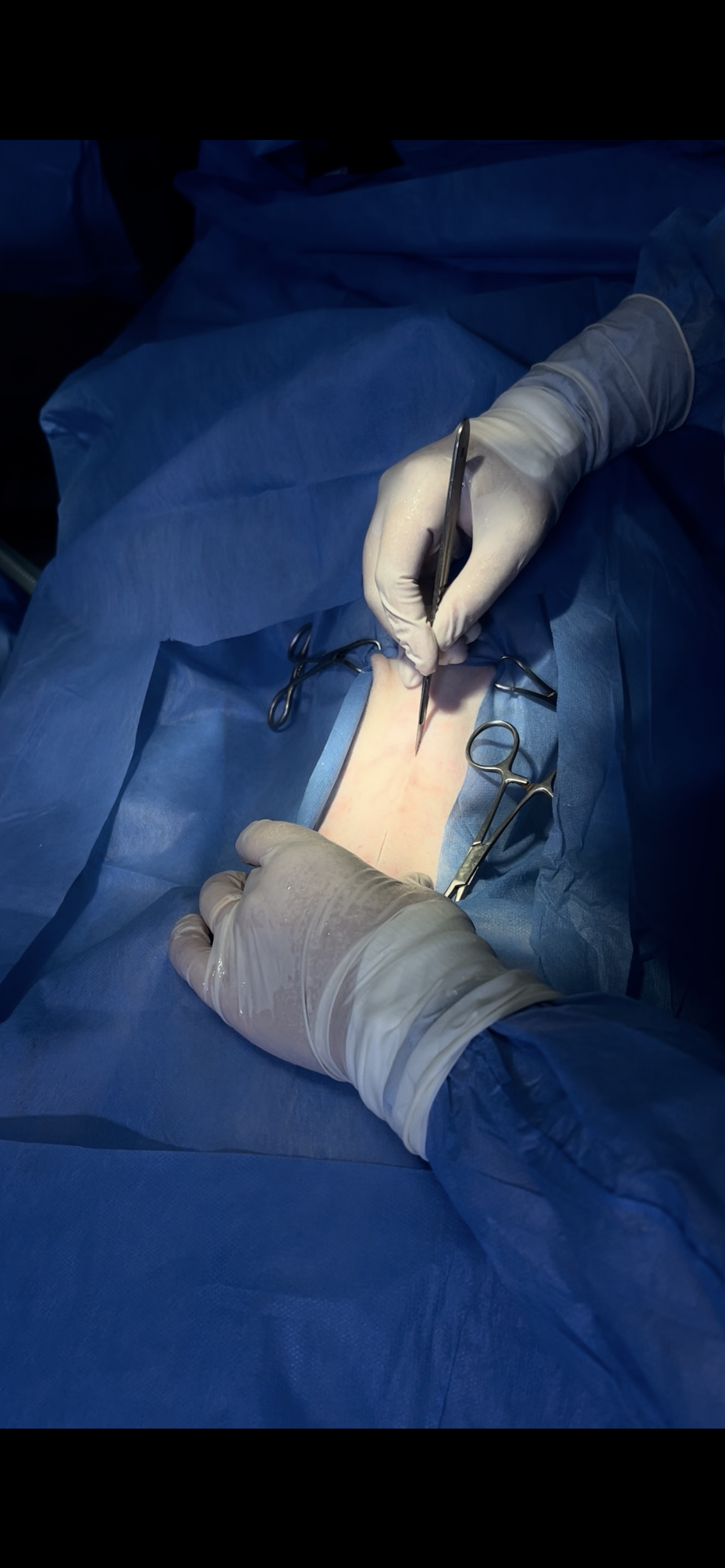
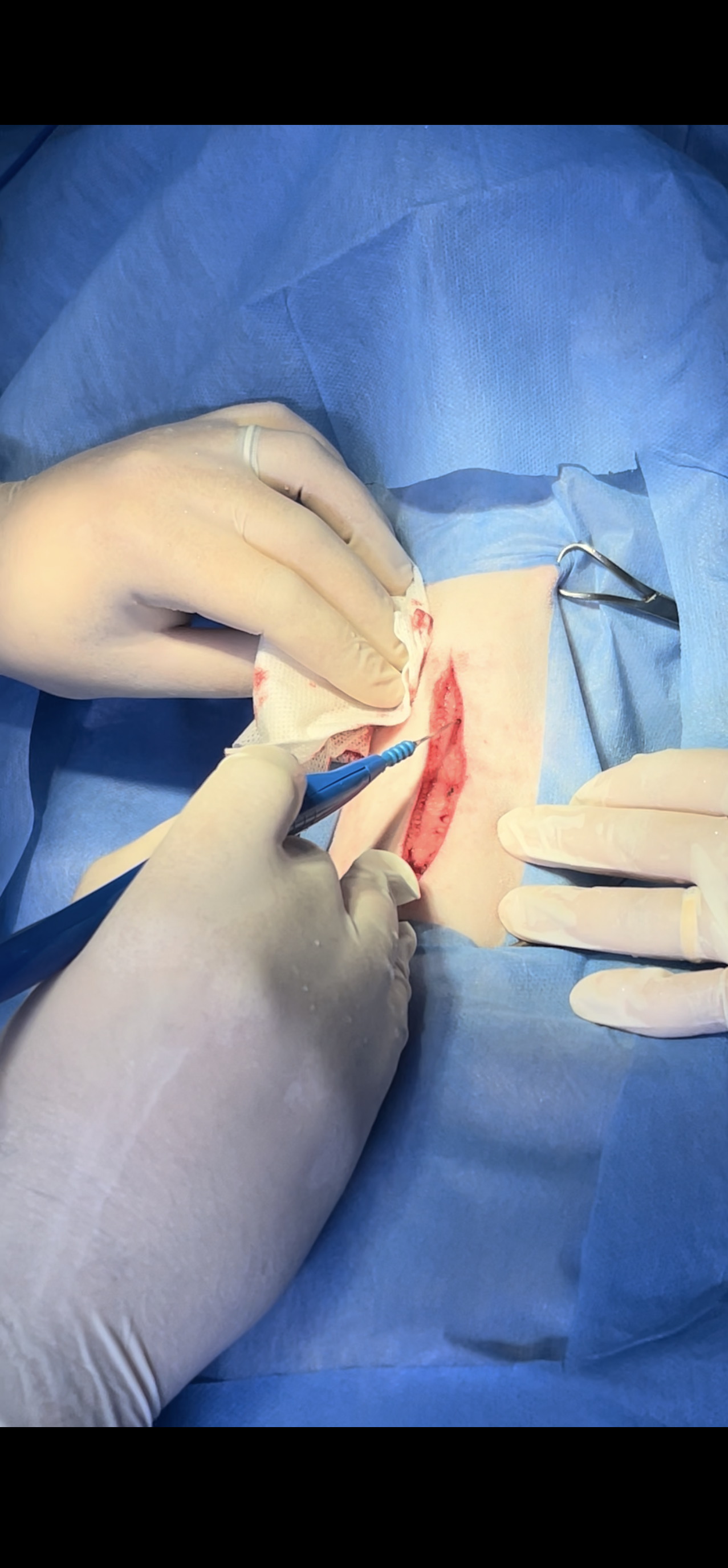
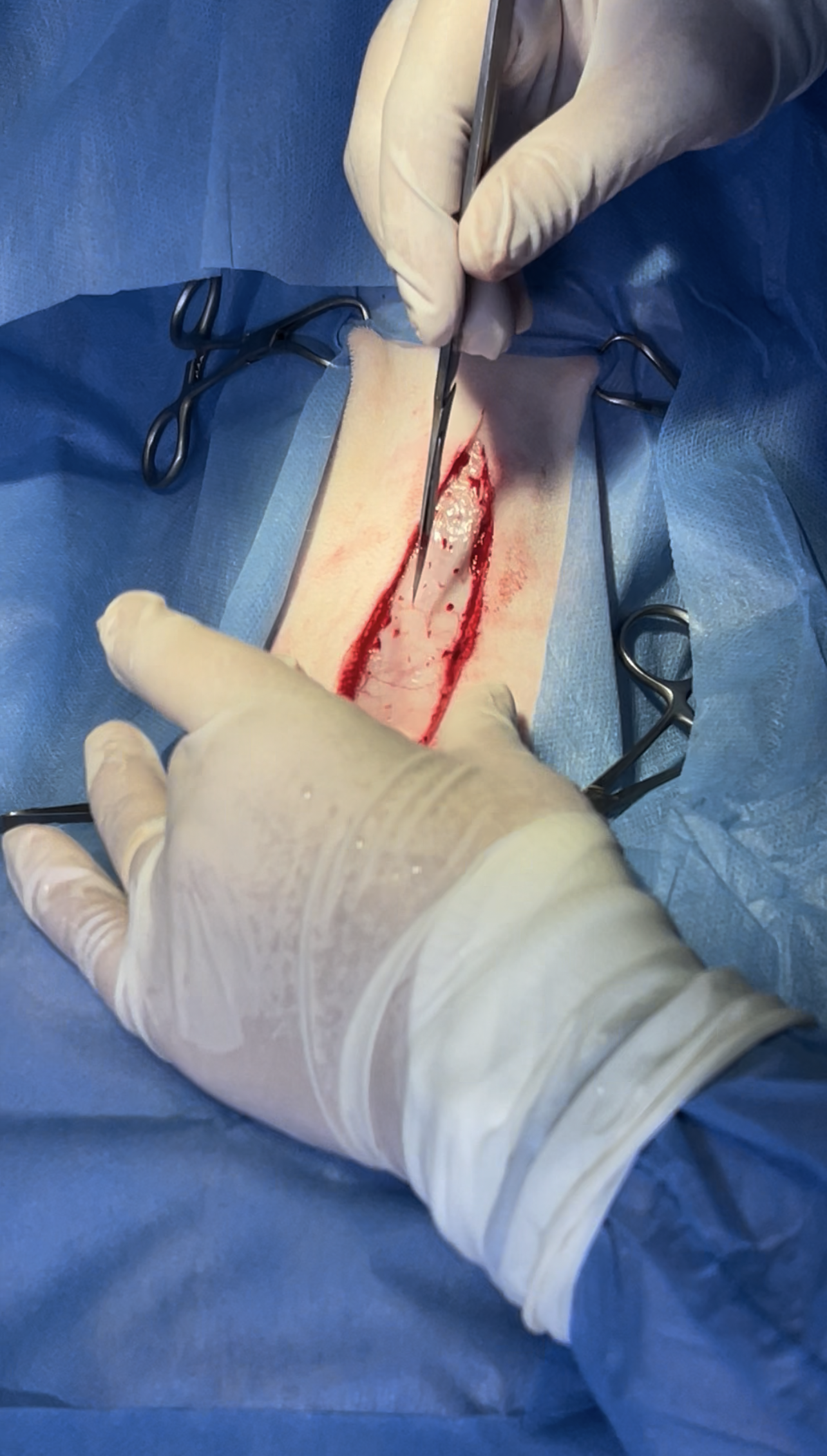
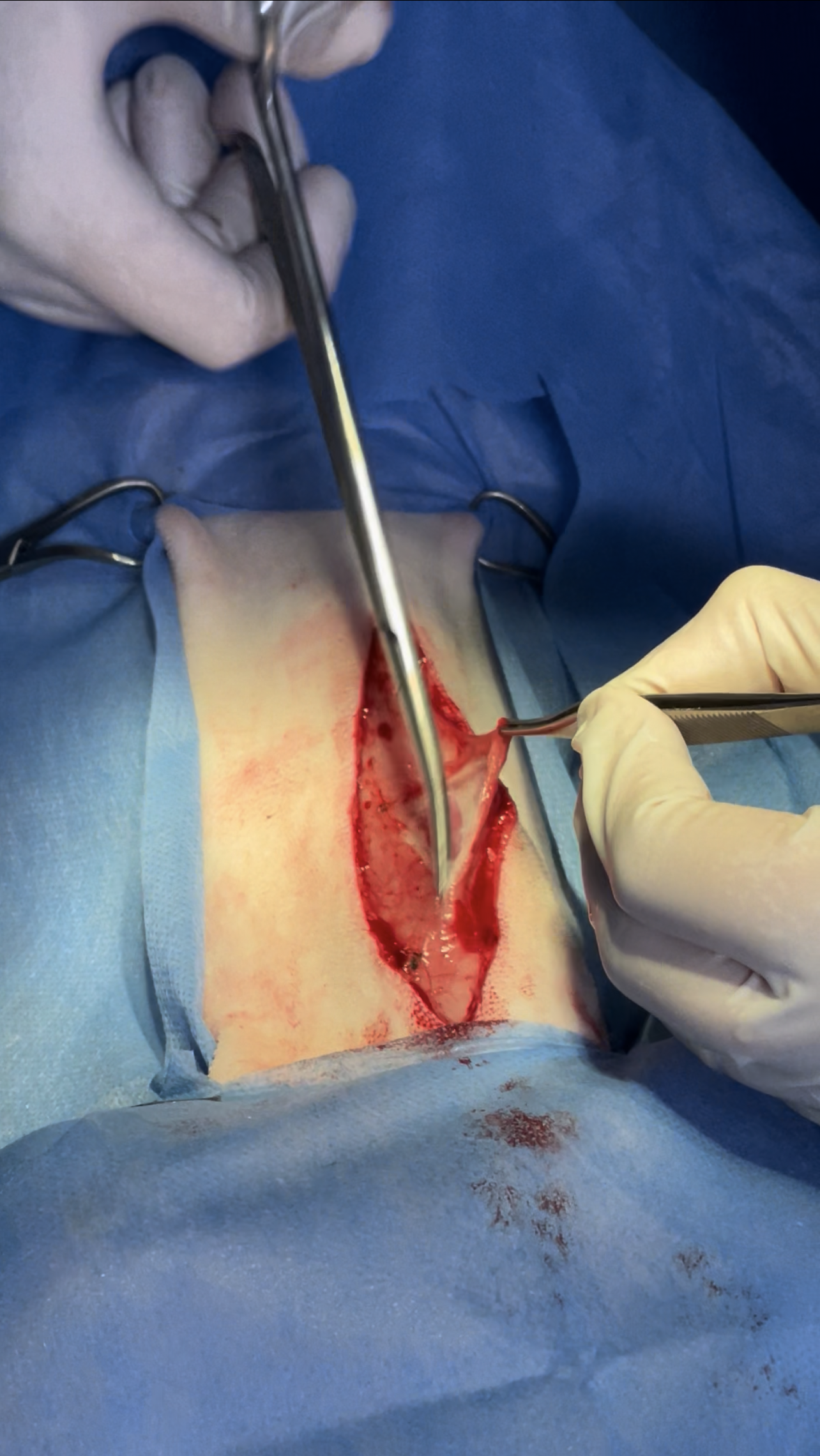
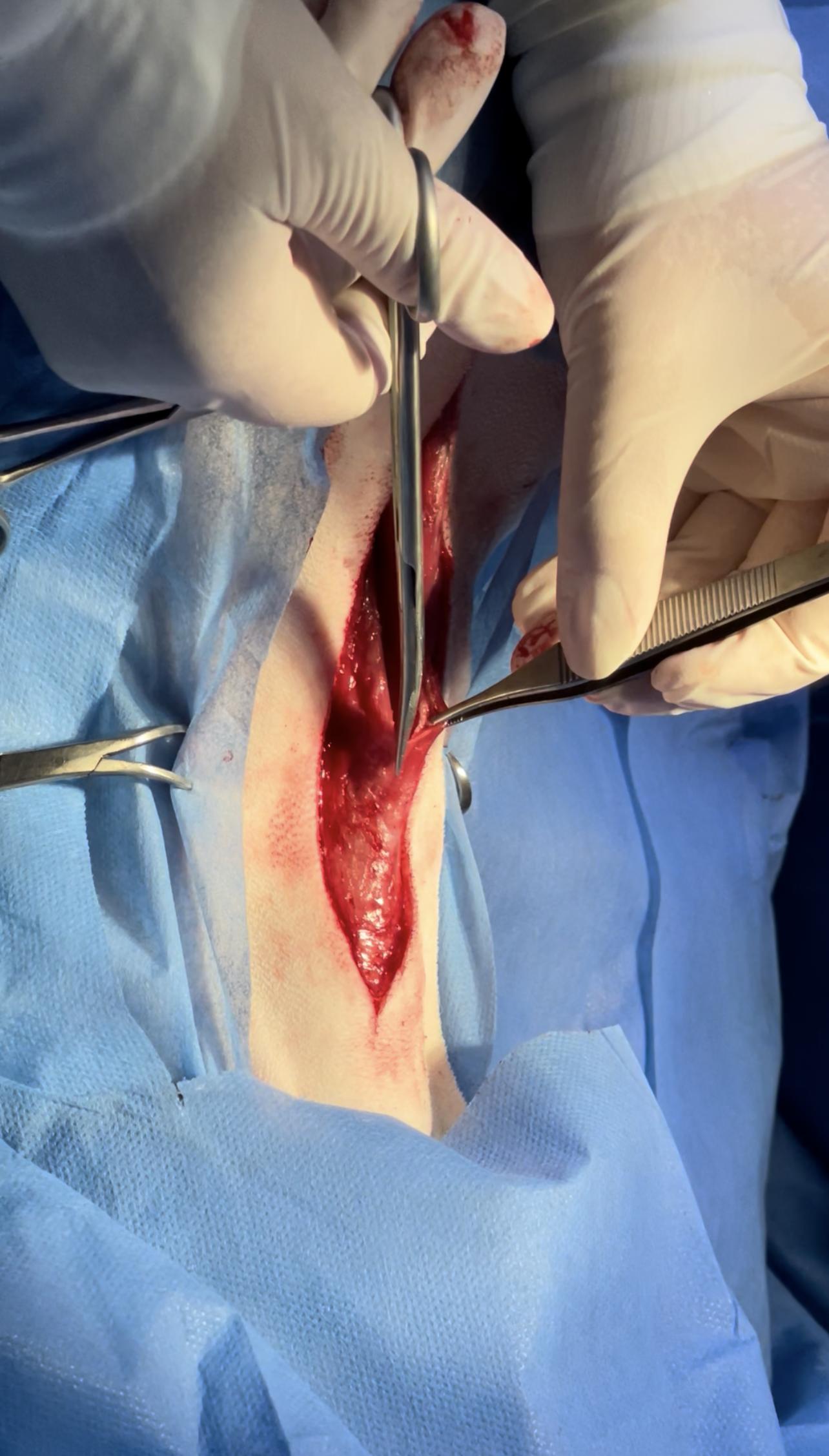
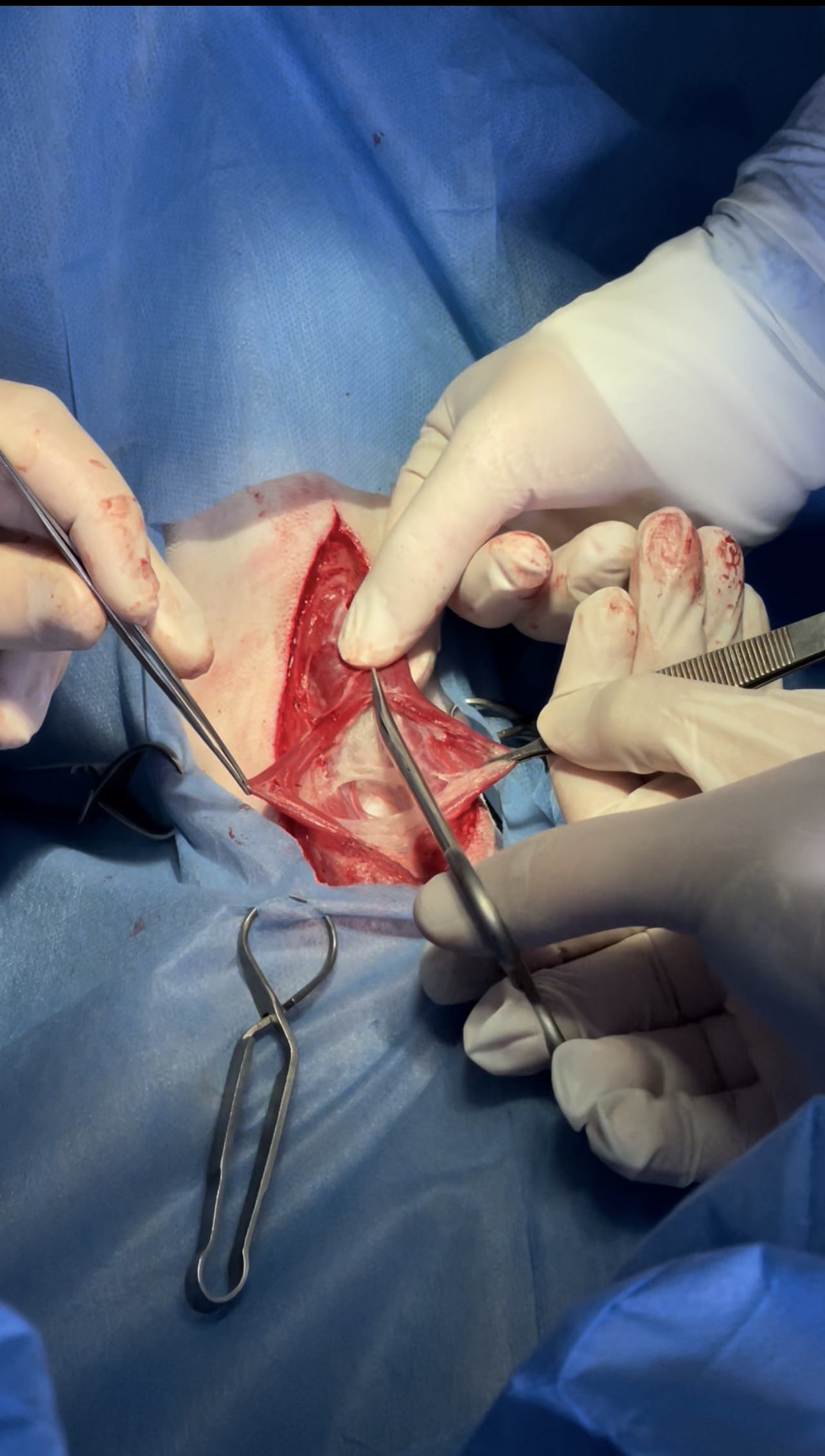
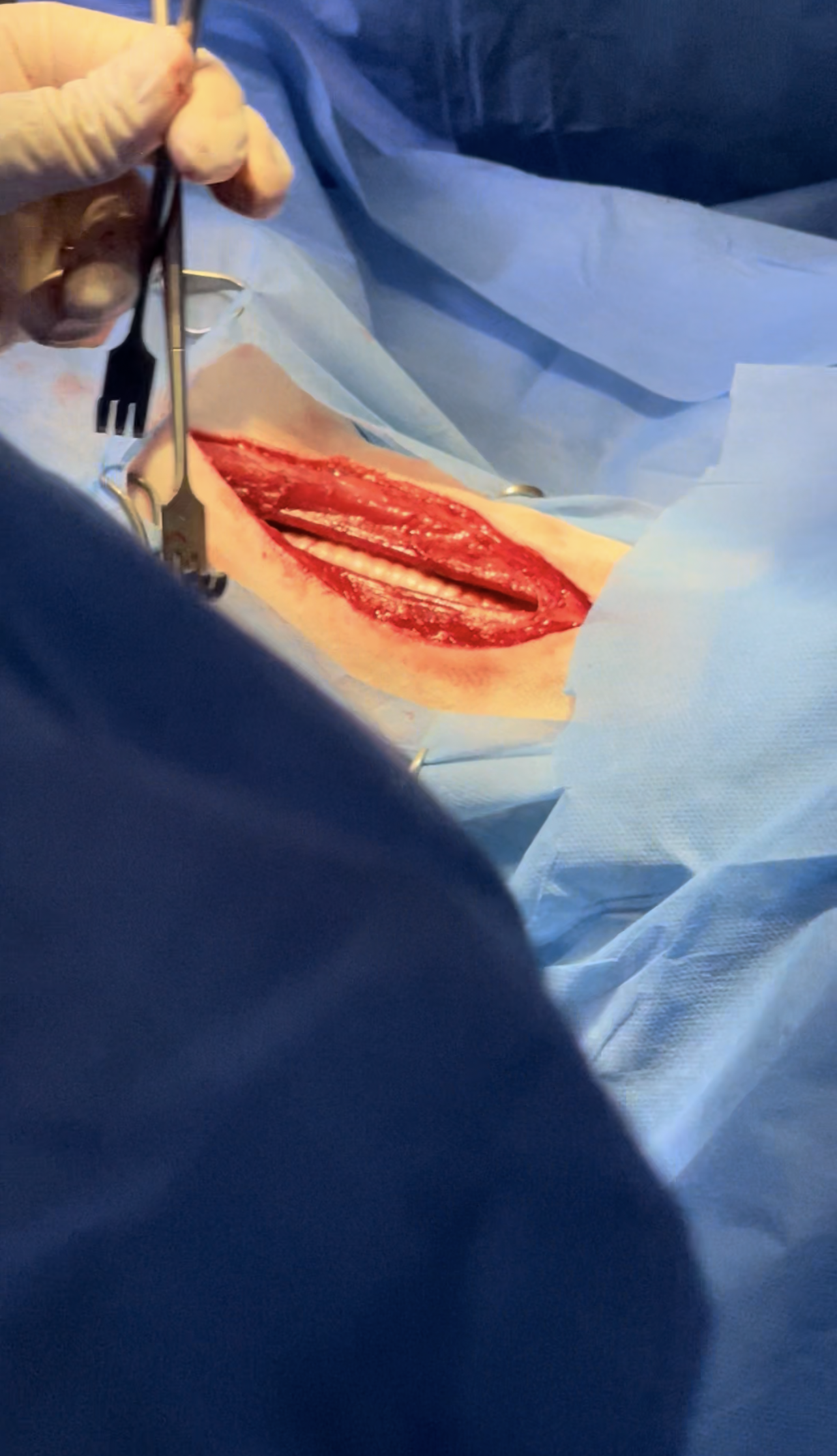
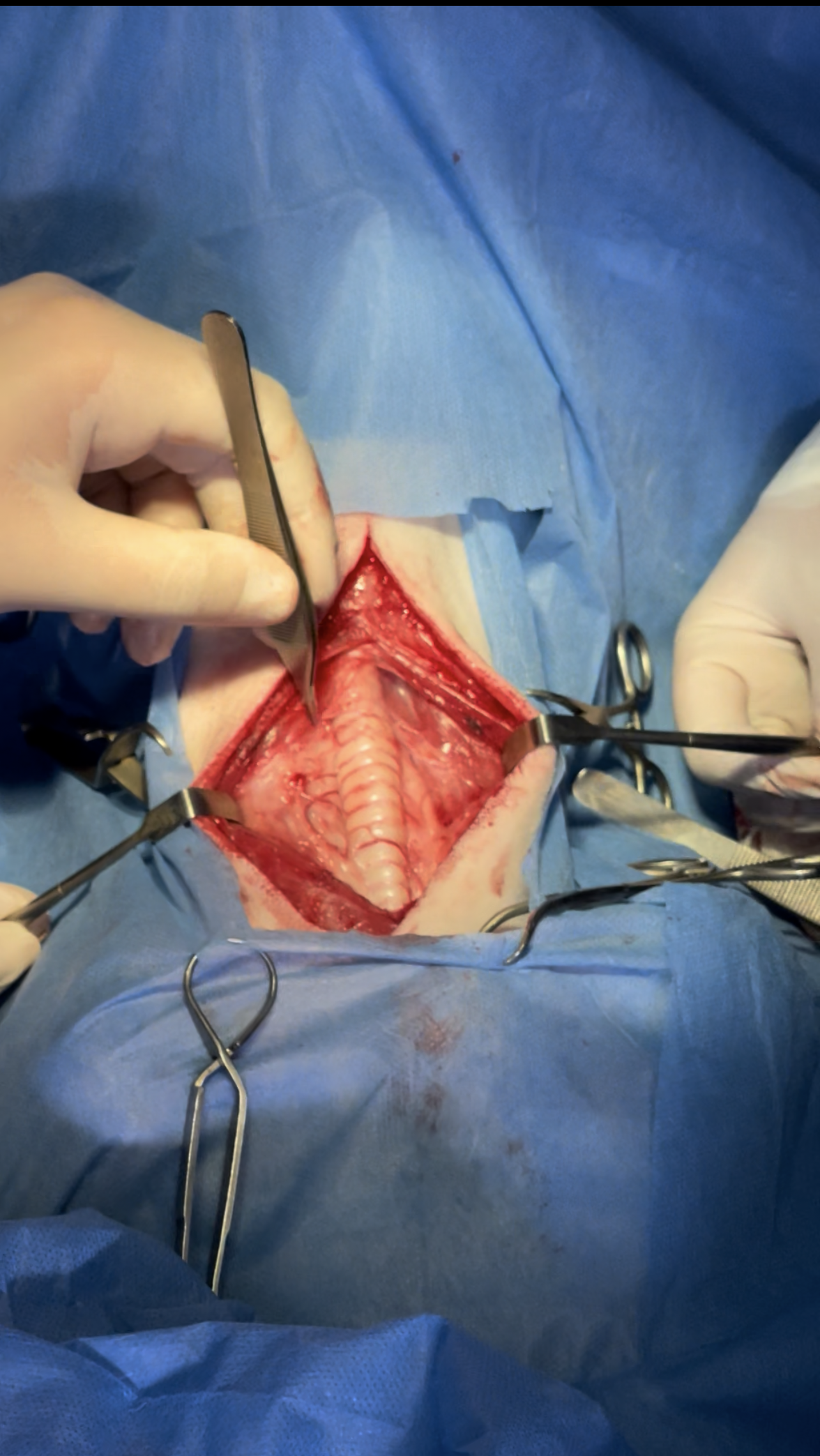
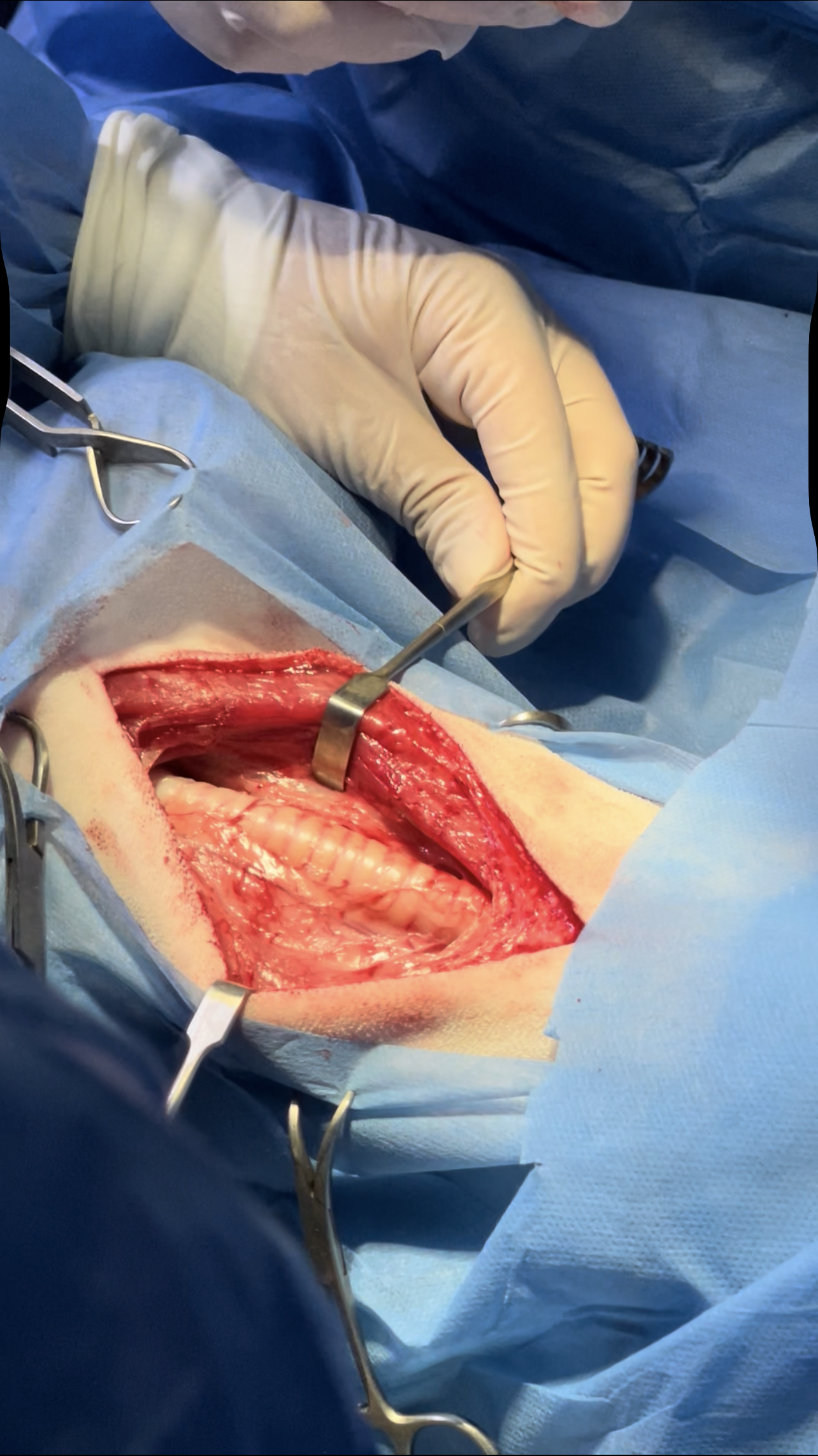
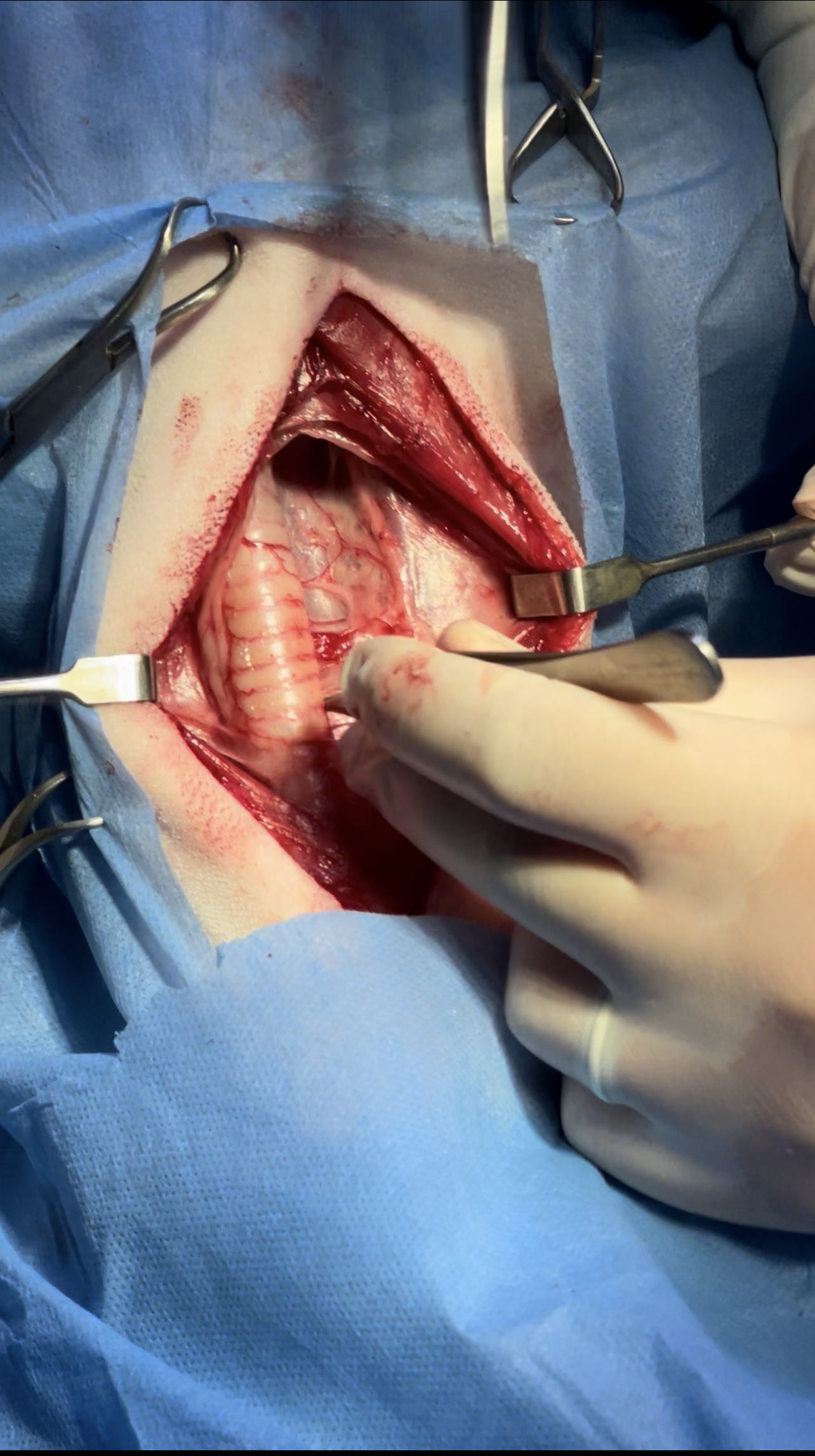
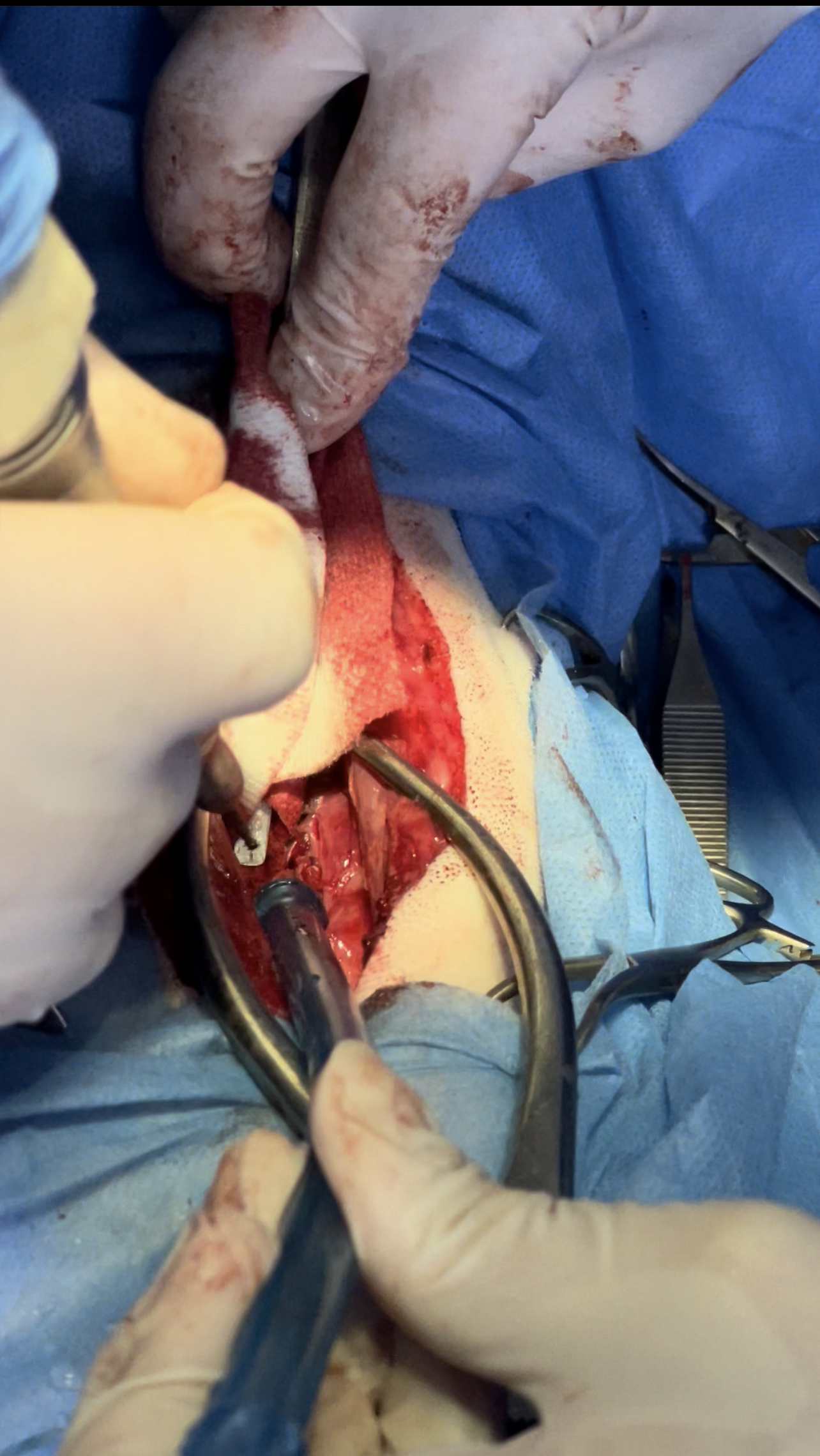
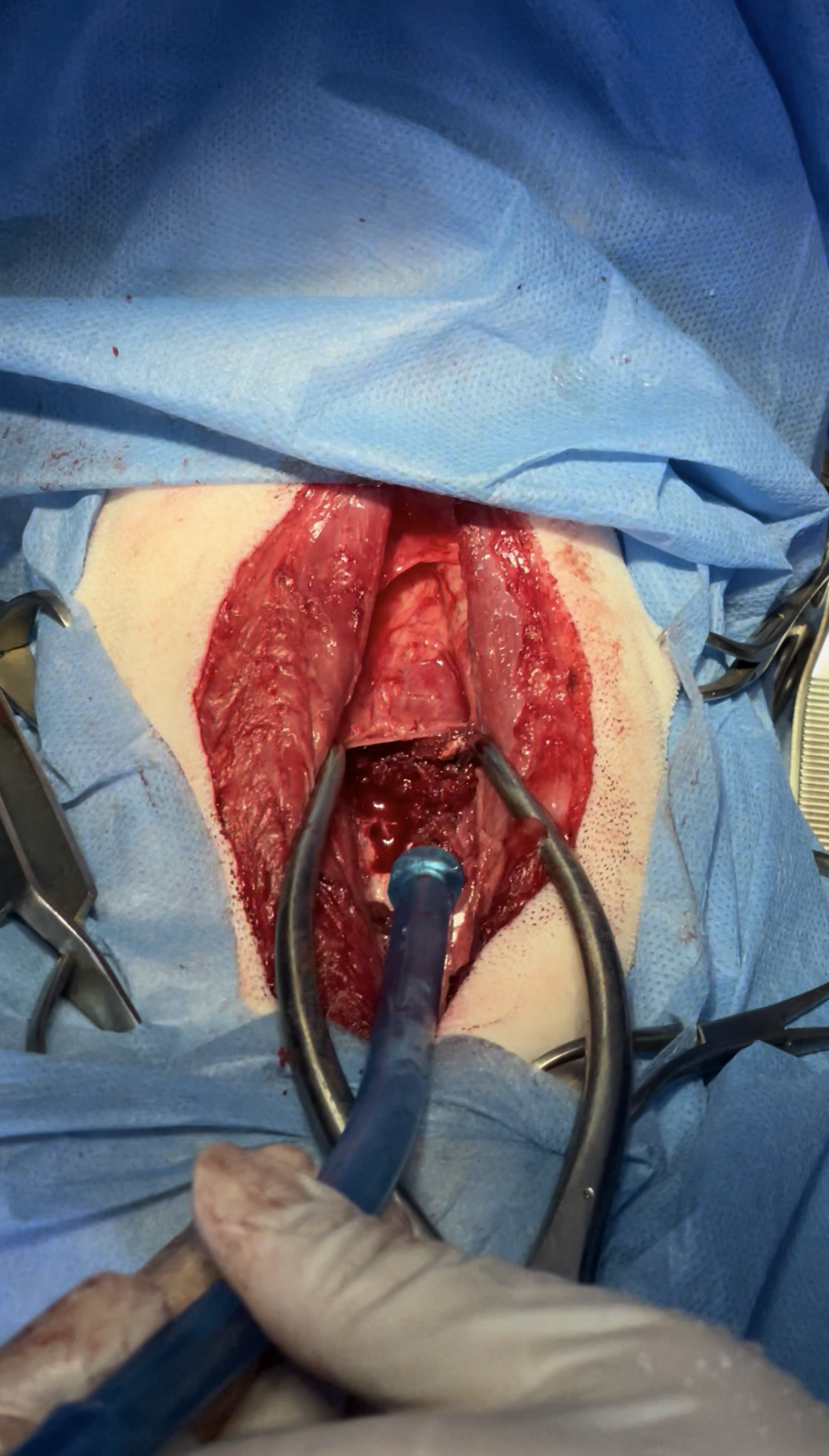
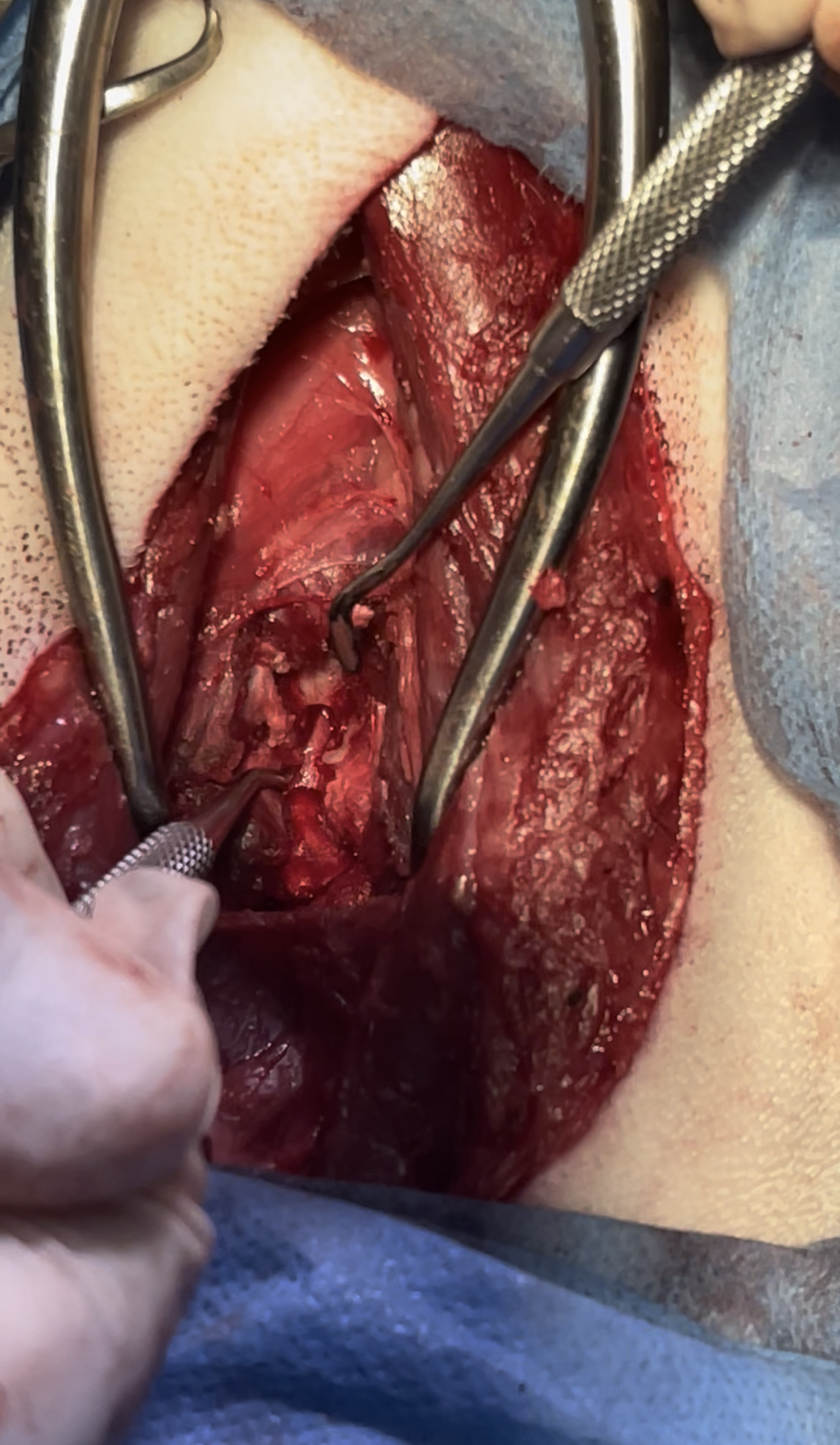
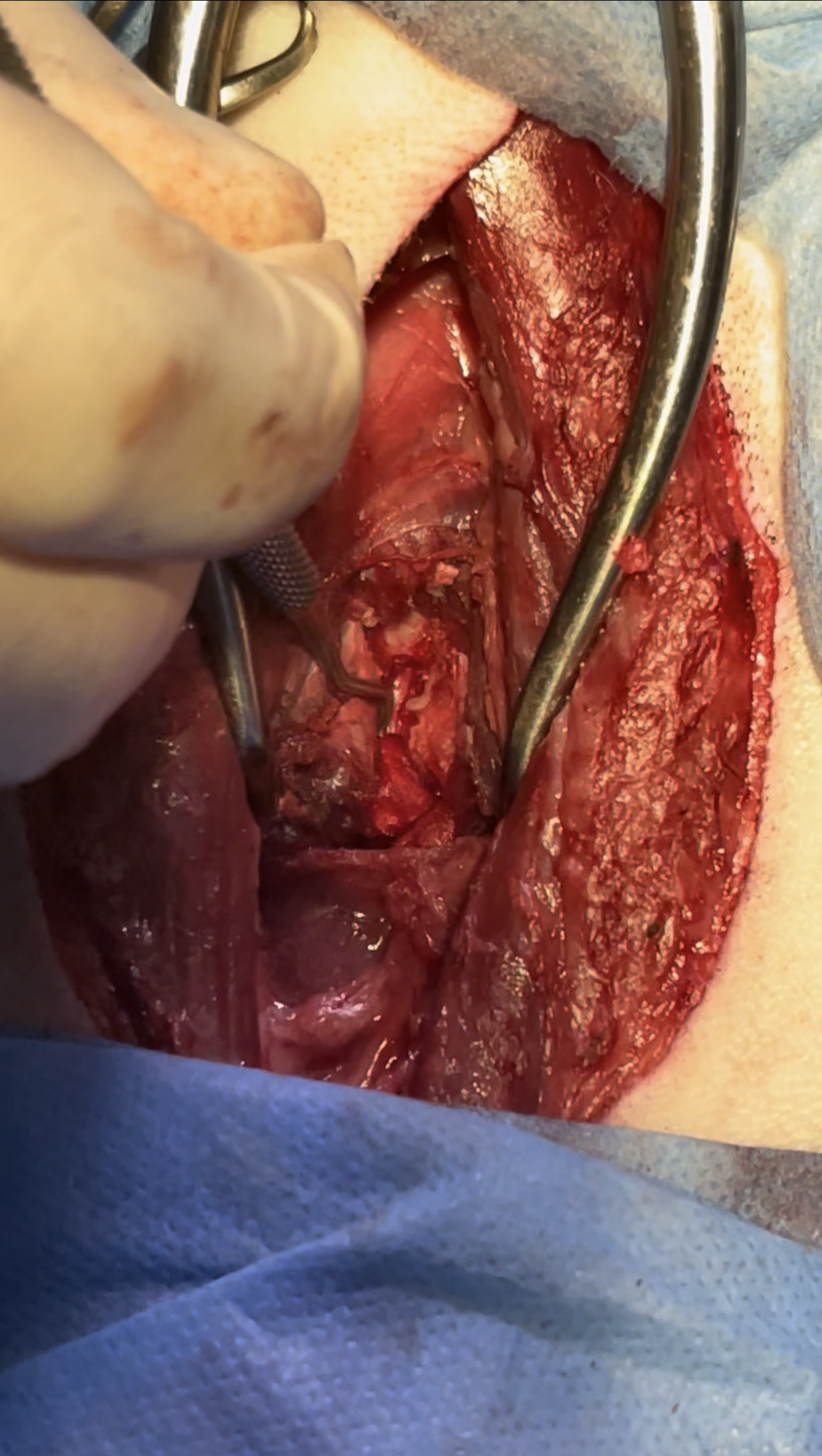
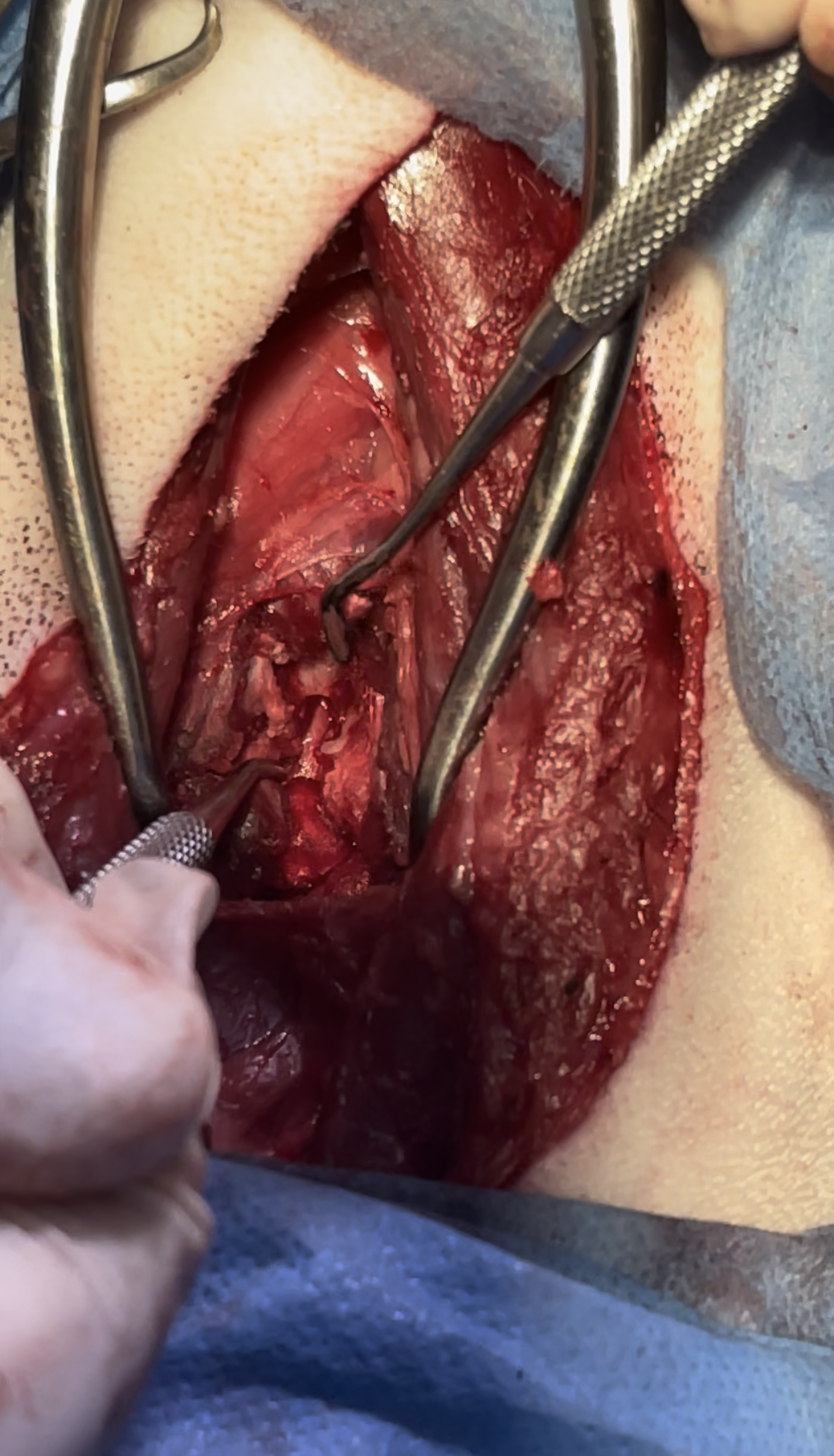
Zeus admitted to surgery Ventral slot approach was planned for removal of extruded disc material and decompression of the spinal cord surgery went successfully and he was able to take his first steps one day after the operation and regain his ability to walk after 3 days
Approach to Cervical Vertebrae C2-C7 Through a Ventral slot :
.
.

.
.

.
.
.
.
.
.
.
.
.

.
.
.
.
.
.
© All Rights Reserved